

Section: New Results
Assisted Grasping in Individuals with Tetraplegia: Improving Control through Residual Muscle Contraction and Movement
Participants : Lucas Fonseca [UnB, Brazil] , David Guiraud, Charles Fattal, Christine Azevedo, Arthur Hiairrassary, Camilo Silva, Anthony Gélys [Propara Rehab. Center, Montpellier] .
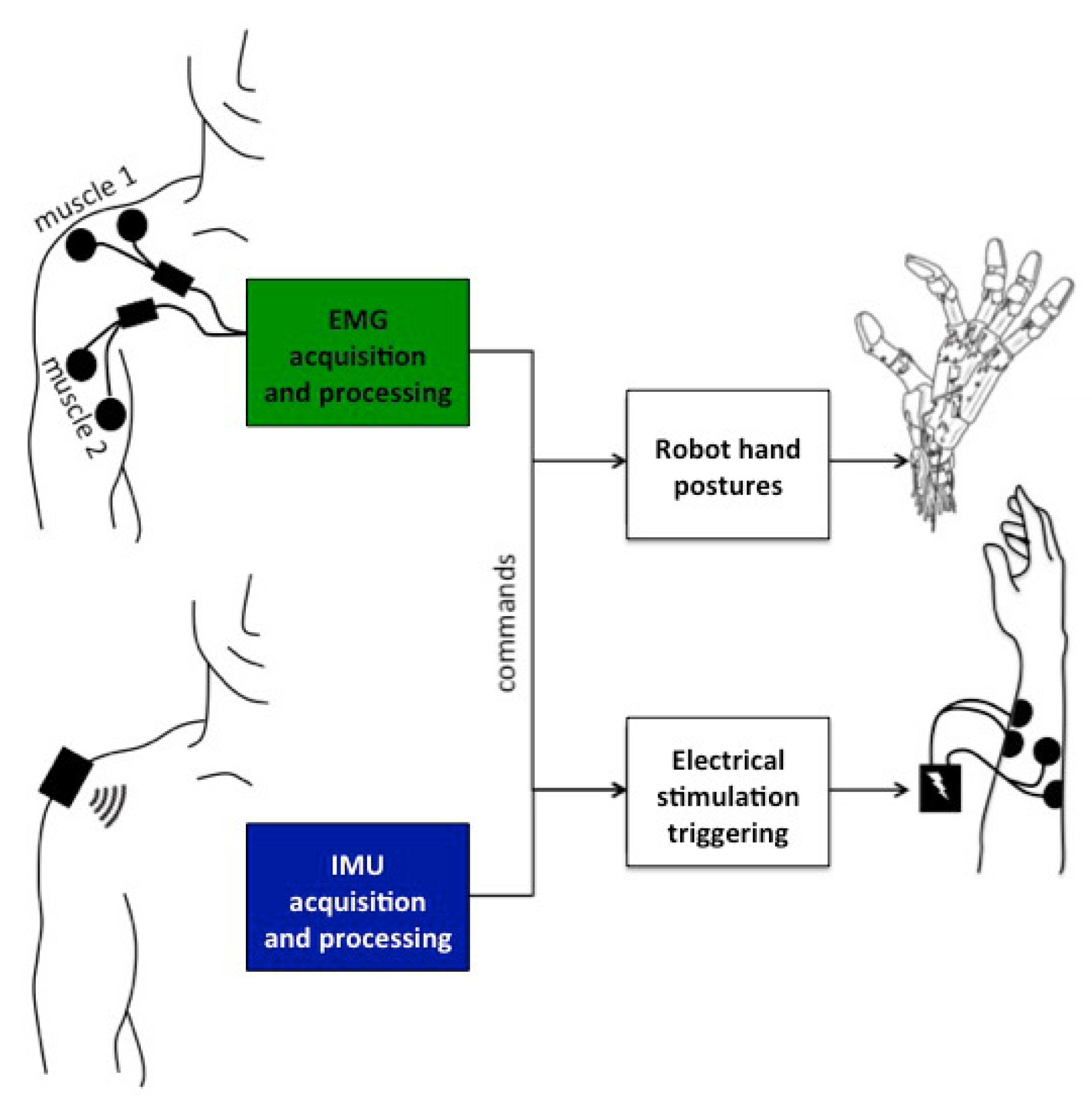
Individuals who sustained a spinal cord injury often lose important motor skills, and cannot perform basic daily living activities. Several assistive technologies, including robotic assistance and functional electrical stimulation, have been developed to restore lost functions. However, designing reliable interfaces to control assistive devices for individuals with C4–C8 complete tetraplegia remains challenging. Although with limited grasping ability, they can often control upper arm movements via residual muscle contraction. We have explored the feasibility of drawing upon these residual functions to pilot two devices, a robotic hand and an electrical stimulator. We studied two modalities, supra-lesional electromyography (EMG), and upper arm inertial sensors (IMU). We interpreted the muscle activity or arm movements of subjects with tetraplegia attempting to control the opening/closing of a robotic hand, and the extension/flexion of their own contralateral hand muscles activated by electrical stimulation. Two groups of participants with quadriplegia were recruited (Clinique Propara, Montpellier): eight subjects issued EMG-based commands; nine other subjects issued IMU-based commands. For each participant, we selected at least two muscles or gestures detectable by our algorithms. Despite little training, all participants could control the robot’s gestures or electrical stimulation of their own arm via muscle contraction or limb motion [20].
|
In the AGILIS project supported by EIT Health, we intend to extend this approach to participants with 2 implanted electrodes on median and radial nerves participating in a 30-days clinical study (APHP, Paris and Clinique La Châtaigneraie, Menucourt).
We are currently working on the software that is responsible for acquiring sensor data and controlling the stimulator (§5.2.4). The previous algorithms are being implemented in a single platform focusing on the 30-days clinical study. The residual motion based system was improved based on the results published in [20]. It is also faster and more efficient. The inertial sensors now have higher frequency, which leads to higher accuracy of movement classification, particularly with faster movements.