Section: New Results
Function control and synthesis
FES assisted sitting pivot transfer
Participants : Jovana Jovic, Christine Azevedo Coste, Philippe Fraisse, Sebastien Lengagne, Charles Fattal.
Transferring from a wheelchair to a treatment table, bed, tub/shower bench, toilet seat, car seat and vice versa represent typical Sitting Pivot Transfer (SPT) realized by individuals with Spinal Cord Injury (SCI). Individuals with SCI, perform this postural task around fifteen times a day using upper extremities. In the chronic stage after SCI, soft tissue structures are exposed to overuse in activities of daily living, such as, transfer task in which the shoulder becomes a weight-bearing joint. Therefore, the risk of shoulder pain and musculoskeletal disorders is higher in persons with paraplegia compared with an able-bodied population. A lot of scientific effort has been focused on experimental studies in which the kinetic and the kinematic of the SPT movement have been analyzed. To our best knowledge, the scientists have focused their attention only on the performance of SPT; the influence of Functional Electrical Stimulation (FES) on SPT maneuver has not been investigated so far.
Therefore, we investigate the influence of FES on SPT motion of a paraplegic person. First, we develop dynamic optimization method in order to predict SPT motion of an able-bodied subject. This approach have been validated by comparing computed SPT trajectories with the ones measured during the experiment with an able-bodied subject (see Fig. 7 ). After validating our method, we used the optimization tool for analyzing the influence of FES on SPT maneuver in paraplegic persons. Our results suggest that FES can decrease arm participations during the transfer motion of a paraplegic person. [6] , [21] .
|
FES assisted prolonged standing
Participants : Jovana Jovic, Philippe Fraisse, Christine Azevedo Coste, Charles Fattal.
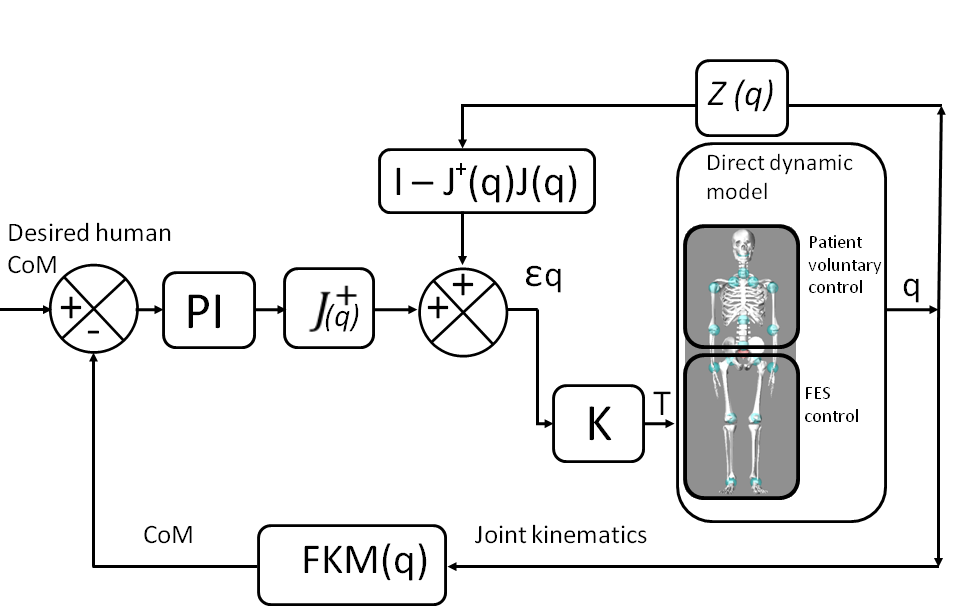
Prolonged immobilization which occurs after spinal cord injury results in many physiological problems. Standing therapy can ameliorate many of those problems. The approaches proposed in the literature for restoration of standing in paraplegic population based on Functional Electrical Stimulation (FES) focuse on the control of each individual joint, i.e. joint space control. In those cases the balance of the postural system is not directly controlled. This could be problematic especially when only the lower limbs are controlled. During paraplegic's quiet standing two concurrent controllers are acting in parallel, the physiological system under control of Central Nervous System (CNS), and artificial FES system. Upper part of the paraplegic's body is under voluntary control, therefore artificial controllers should be designed in the way to take into account actions of the intact part of the body and to assist users in their task.
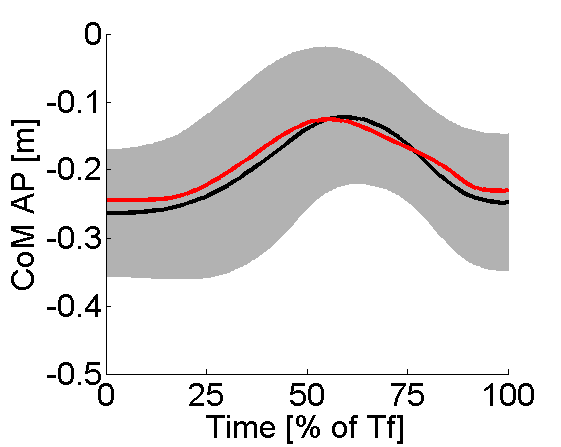
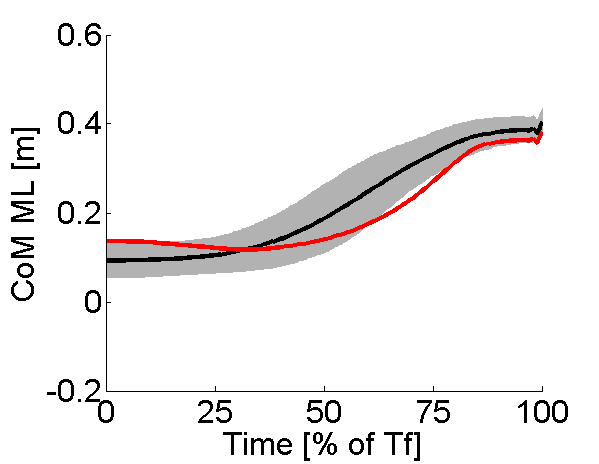
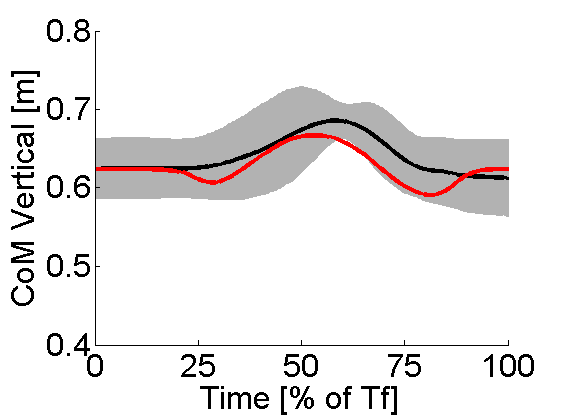
For human beings the Center of Mass (CoM) provides an indicator of stability and it is an essential parameter in human postural stability. By controlling CoM position in paraplegic person the voluntary motions under CNS control are taken into account. Therefore, in we propose a whole body controller based on control of the CoM position. The goal was to develop a simple balance controller which would, by means of FES, enable quiet standing of individuals suffering from SCI while taking into account the voluntary motion of the upper limbs. The controller should enable prolonged standing by simulating the behavior of an able-bodied subject during the standing task, i.e. by imposing posture switching and in that way allowing the stimulated muscles to relax. The proposed approach is based on a 10 DoF biomechanical model and Proportioan Integral (PI) controller (see Fig. 8 ). The validity of the approach is tested, in computer simulations, using human CoM trajectories estimated from experimental data and by applying perturbations in simulation during quiet standing in order to simulate voluntary upper body movements.The results show that proposed controller is able to track desired CoM position with sufficient precision and to maintain stability even in the presence of simulated movements of the upper body [20] .
|
Bimanual reeducation assisted by FES in post-stroke patients
Participants : Nader Rouis, Christine Azevedo Coste, Philippe Fraisse, Isabelle Laffont, Denis Mottet.
This starting project will investigate the possibility to stimulate the deficient upper limb of a post-stroke patient in order to reproduce the movements observed on the valid upper limb or in order to achieve a bimanual task in cooperation with the valid upper limb. The aim is to improve the bimanual training tasks classically used in fictional rehabilitation. Both embedded sensors and kinect type systems will be investigated as possible ways to observe the valid upper limbs.
Freezing detection in Parkinson Disease patients
Participants : Maud Pasquier, Christine Azevedo Coste, Christian Geny, Bernard Espiau.
This work intends to apply the results of Maud Pasquier thesis about data segmentation and locomotion analysis to the detection as soon as possible of freezing episodes in Parkinson Disease (PD) patients. PD is a chronic degenerative disease of the central nervous system. One of the consequence is walking troubles and increased postural instability and falling risks. Freezing concerns at least half of PD patients, it is characterized by the transitory incapacity to make a step. It classically occurs at the gait initiation, turn around and passing doors. This freezing of gait (FOG) strongly impacts patient's mobility. As an example, in figure 9 , data recorded by an inertial sensor placed at the ankle is presented.
|
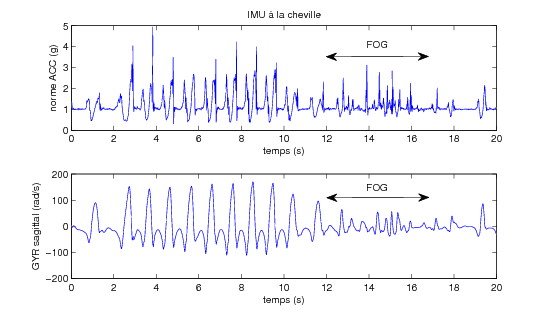
Assistive devices have been proposed, it has been shown that providing the patient with an auditory metronome or visual lines on the ground allows to reduce FOG occurrence but the effects are not maintained within the time. An approach would be to present this signals only when a freezing episode occurs and this implies to be able to detect it. Several authors have shown that FOG are in general associated to walking rhythm variability. Moore et al have used an accelerometer placed on lower limv in order to detect the presence of high frequencies. Indeed, the tremor pattern which can be observed during freezing is located at 3 et 8Hz, whereas normal locomotion is around 3Hz. These authors are able to detect a large part of the FOG but only those presenting high frequency patterns which is not systematic. Furthermore the detection delay (FFT) is very high and cannot be compatible with assistive device control constraints. We have proposed to observe stride properties in an online manner and compute a criterion which value informs about the FOG occurrence. The criterion is based on two variables: the stride length and the cadence. When stride length diminishes and cadence increases a FOG may be upcoming. 3 patients have been involved in this study and the criterion proposed has been shown to be as efficient than Moore's method in terms of number of detected FOG but the detection time is strongly improve with our method.
"Awake surgery" of slow-growing tumors and cortical excitability measured by EEG recordings.
Participants : François Bonnetblanc, Guillaume Herbet, Pom Charras, Mitsuhiro Hayashibe, David Guiraud, Hugues Duffau, Bénédicte Poulin-Charronnat.
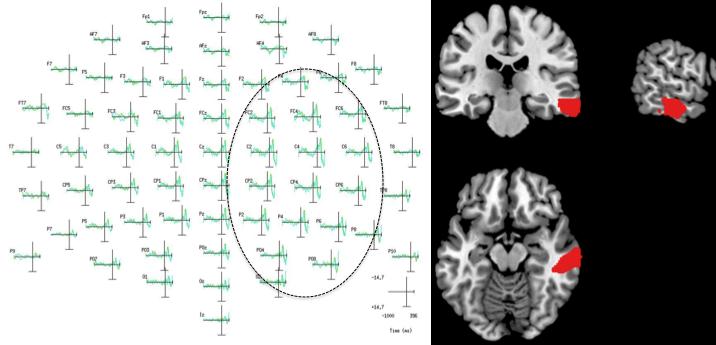
Using direct electrical stimulation, real-time functional mapping of the brain can be used to perform resections of slow-growing infiltrative tumors in awake patients and to prevent the resection of essential areas near the tumor. To investigate interhemispheric imbalance following " awake surgeries" of slow-growing tumors we recorded EEG in a visuo- manual RT paradigm. Increase of cortical excitability within the ipsilesional hemisphere was signed by increased event related potentials (ERPs) amplitude for two patients. The cortical excitability in the lesioned hemisphere may be increased to maintain performances and cerebral plasticity.
|