

Section: New Results
Assistance
We are still going on in building a framework for customizable and modular assistive robotics including hardware, software and communication and medical monitoring. The development of our platforms shows that we are now able to identify problematic issues for end-users, helpers and the medical community and to propose appropriate hardware/software solutions. But the most time consuming part of our work is related to evaluation and therefore experimentation: this involves legal/ethical issues (for which we have contributed [5]), participation of the medical community (for evaluation and recruitment) and heavy administrative management. Clearly we are lacking of permanent staff as we have long term objectives that cannot be fulfilled only with PhD or post-doc students. We need also engineers during specific periods (for hardware development and experimentation) but over a longer time than the one or two years currently proposed by Inria.
Rehabilitation in an immersive environment
Participants : Artem Melnyk, Jean-Pierre Merlet, Yves Papegay [correspondant] , Ting Wang.
Rehabilitation is a tedious and painful process and it is difficult to assess its trend. Using an immersive environment has shown to increase the patient motivation but is not sufficient regarding rehabilitation efficiency. First the visual feedback (event 3D) is not sufficient to provide a full immersive feeling as body motion is not involved. Controlling body motion is also very important for therapists that currently must continuously correct the patient pose so that the rehabilitation exercise is the most efficient. We propose to add motion generators in the environment to reinforce realism (thereby increasing patient motivation) but also to allow therapists to use these generators to control the body pose so that they will be able to repeat rehabilitation exercises in a controlled context. Furthermore these generators are instrumented to provide information on the body pose and additional external sensors complete these measurements for rehabilitation assessment. We have developed 3 types of motions generators: one 6 d.o.f. motion base, a CDPR that is able to lift a patient and 2 multipurpose lifting columns.
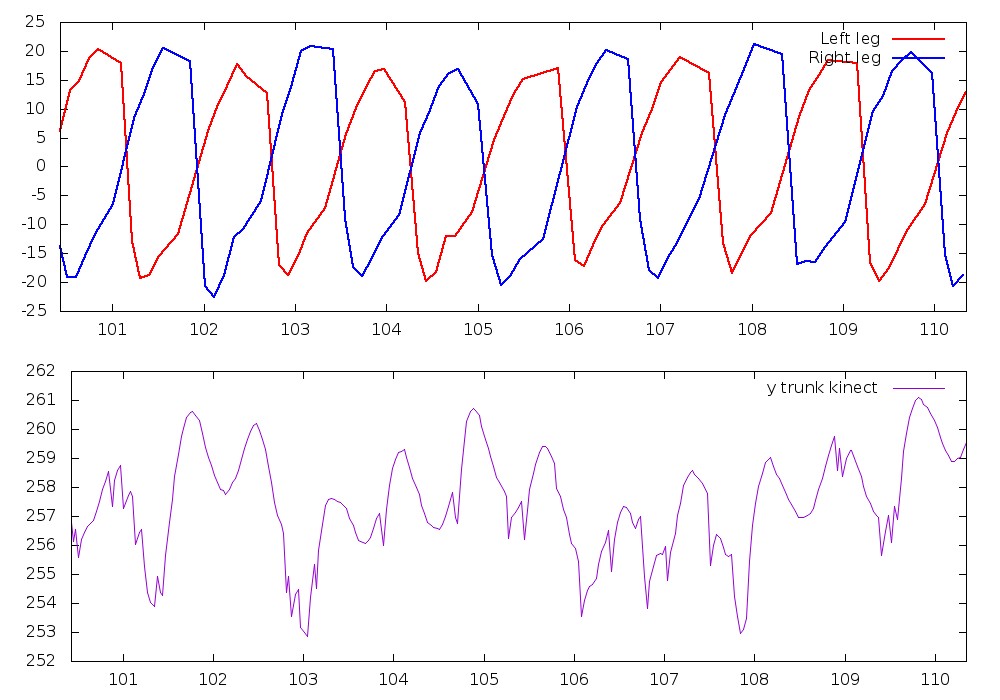
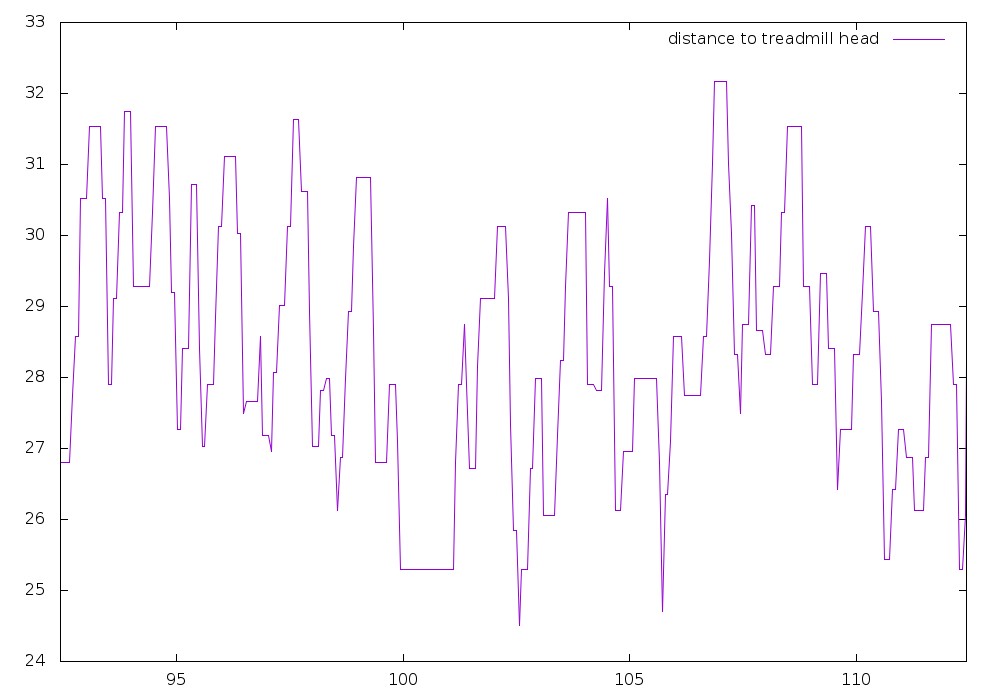
When starting this project we were planning to use Inria-Sophia immersive room , hence allowing us to focus on the rehabilitation station. Unfortunately this room is no more available. This year we have developed a 2D renderer that has been connected to a flexible software platform allowing the various agents to exchange messages. We have been able to build a first version of our rehabilitation platform using a treadmill as exercise tool and columns to animate the treadmill (figure 1). For measuring the gait pattern we are using a planar lidar for detecting the leg motions, a kinect for detecting the motion of a skeleton and a distance sensor that measure the body motion with respect to the head of the treadmill. Figures 2 and 3 show an extract of the measurements obtained during a typical walk. It may be seen that the lidar data are very clean and allows one to estimate the mean position of the leg as a function of time (from which we will be able to deduce the number of steps, velocities of the leg, ...). Kinect data are much more noisy although that a fusion with the lidar data and the distance data will allows us to detect significant trunk motion. A typical walk of 3mn provides approximately 20 Mo of data.
|
|
Note that we are not using wearable sensors (although they are available: accelerometers for the arms and legs, shoes with pressure sensor and accelerometers): this is voluntary as our contacts with the medical community have indicated that many patients will not be comfortable with wearable sensors. In the same manner we have experimented having a headset instead of the screen but it appears that visualization is very disturbing and uncomfortable. Subject safety is ensured: during the exercise the subject must keep a push button pressed and when released the treadmill stop immediately. An emergency stop button is also available for the operator. Furthermore the system has been designed to provide various supports for avoiding fall and is surrounded by soft carpets.
The rehabilitation station for walking analysis on a treadmill in various walking condition is now almost fully functional and reliable. The next step will start of the beginning of 2019 with an experiment involving a cohort of voluntary subjects of Inria in order to obtain a significant amount of data. A statistical analysis of these data will then be performed in order to examine if synthetic and medically pertinent indicators (besides classical indicators such a number of steps, velocity, ...) may be obtained. The next step will involve repeating this experiment with pathological patients from Centre Héliomarin de Vallauris, most probably at the end of 2019. Meanwhile we will integrate our motion base as another element of the rehabilitation station with the purpose of equilibrium analysis, using a sea landscape as virtual environment with fans providing a realistic simulation of winds.