

Section: New Results
Function control and synthesis
Correction of drop-foot in post-stroke hemiplegic patients
Participants : Christine Azevedo Coste, Roger Pissard-Gibollet (SED INRIA), Fabien Jammes (INRIA RA), Jérôme Froger (Rehab. Centre, Grau du Roi, CHU Nîmes).
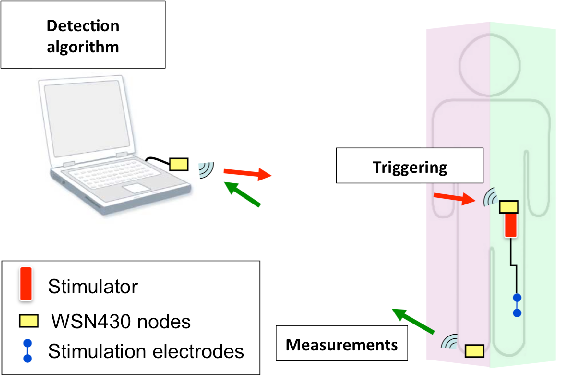
Hemiplegia is a condition where one side of the body is paretic or paralyzed; it is usually the consequence of a cerebro-vascular accident. One of the main consequences of hemiplegia is the drop-foot syndrome. Due to lack of controllability of muscles involved in flexing the ankle and toes, the foot drops downward and impede the normal walking motion. Today, there are commercially available assistive systems that use surface electrodes to stimulate Tibialis Anterior (TA) muscle and prevent drop-foot. The efficiency of drop-foot stimulators depends on the timing of stimulation and functionality of dorsiflexion motion. Classically, available stimulators use footswitches to detect foot on/off events. These discrete events allow only for triggering the stimulation and/or playing with the duration of the stimulation pattern, but does not allow for precise online modification of the pattern itself. We have developed algorithms to monitor the ongoing walking cycle by observing the valid limb movements. In order to ensure legs coordination during walking, we propose a robust phase estimation method based on the observer of a nonlinear oscillator. We have modified a commercial stimulator, ODSTOCK, in order to be able to trigger it using our own wireless sensors and algorithms. Agreement from Nîmes CPP (ethical committee) was obtained in June 2010 to run tests on patients. The protocol comprises 1) the control algorithm triggering the stimulator based on signals issued from one wireless inertial sensor placed on healthy shank, 2) a sensor setup including inertial sensors placed on deficient shank and foot, one goniometer measuring deficient ankle angle, one EMG sensor placed on stimulated TA and one instrumented carpet (GAITRITE) (fig.7 ). Several patients have been included in the study and data is being processed [15] [14] .
eEMG Feedback Torque Control in FES
Participants : Mitsuhiro Hayashibe, Qin Zhang, Christine Azevedo Coste.
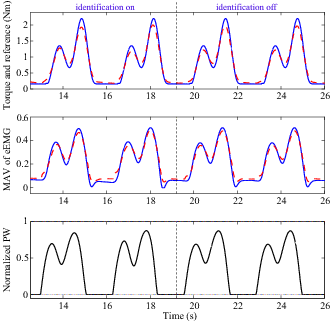
Electrical stimulation (ES) is one of the solutions for drop foot correction. Conventional ES systems deliver predefined stimulation pattern to the affected muscles. However, time-variant muscle response may influence the gait performance as they are difficult to be taken into account in advance. Therefore, closed-loop ES control is important to obtain desired gait in presence of muscle response variation. In this work, a dual predictive control, which consists of two nonlinear generalized predictive controllers, is proposed to track desired torque. The stimulated muscle dynamics are modeled by Hammerstein cascades, with one representing stimulation to activation, the other representing activation to torque. Ankle dorsiflexion torque and ES-evoked EMG of tibialis anterior were recorded experimentally for model identification. The control scheme is validated by following desired torque trajectories with the identified model. The results show that the stimulation pattern obtained from the dual predictive control can produce good torque tracking according to the current muscle condition as shown in Fig. 8 . The updates of model parameters were switched off after certain instant for both the excitation and contraction model. Consequently, the model prediction in the control was only driven by the model input and the last model parameter estimates. The dual predictive controller can still generate suitable control signal to obtain desired torque trajectory [23] .
|
FES assisted Sit-to-Stand
Participants : Jovana Jovic, Christine Azevedo Coste, Philippe Fraisse, Charles Fattal.
Standing up is a common daily activity and a prerequisite to standing or walking. This frequently executed task is one of the most biomechanically demanding activities. The ability to rise from a sitting to a standing position is very important for individuals with paraplegia in order to achieve minimal mobility and has functional and therapeutic benefits related to bone loading, joint extension, cardio-circulatory stimulation, and pressure sore prevention.One method which has been widely investigated is functional electrical stimulation (FES) of the lower extremities. The sit-to-stand method, which is widely used in clinical practice, involves open-loop stimulation of knee extensors activated by hand switches. This technique works adequately in many cases, however, in applying this strategy, stimulation starts without referencespect to the upper body movement. Hence, the whole- body motion is not optimal and requires a high velocity of the joints and large upper limb forces during the rising motion, which may cause both damage of joint tissues and shoulder complications.
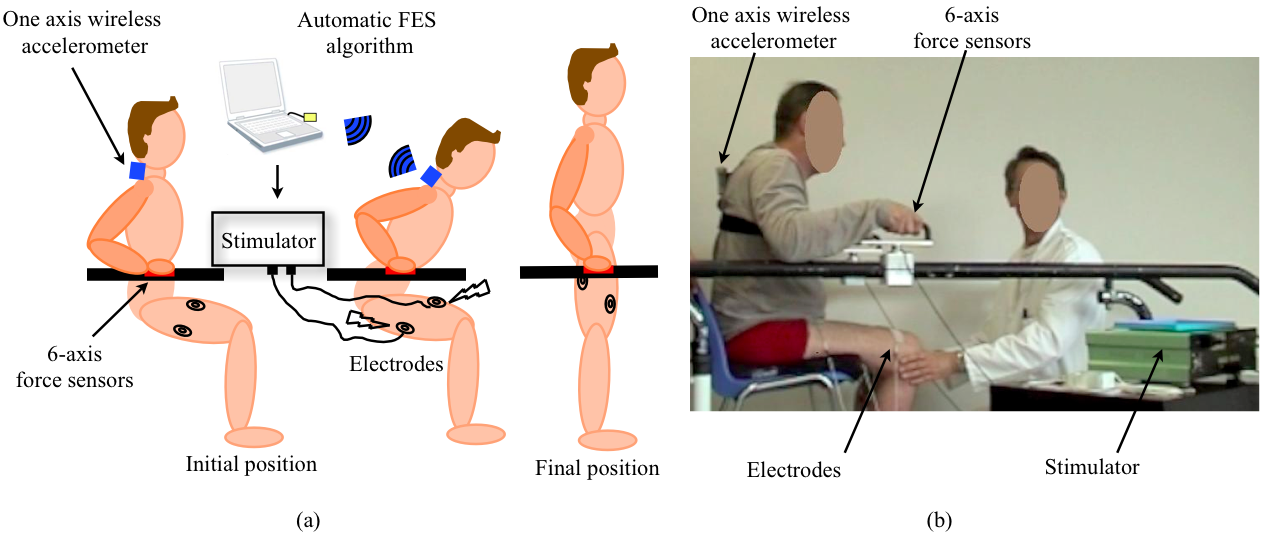
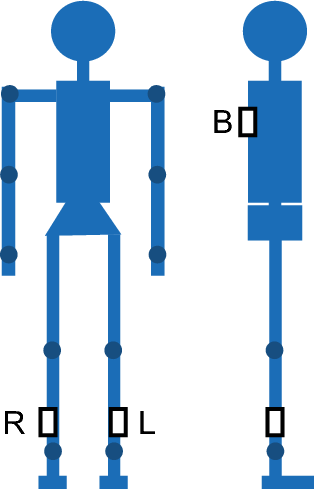
We propose a "patient-driven" FES method that would coordinate motion of the trunk, which is under voluntary control of the patient, and motion of the lower limbs, which are under FES control. The proposed approach is based on the observation of trunk movement during rising motion and a detection algorithm, which triggers a pre-programmed stimulation pattern.Trunk acceleration was acquired by a singleone-axis wireless accelerometer positioned on the subject's back. The detection algorithm consists of an online comparison of the movement acceleration of the ongoing motion with the reference pattern (a typical pattern characterizing the sit-to-stand transfer for each subject) using Pearson's correlation coefficients [25] . Experiments on paraplegic subjects are ongoing in refabilitation center PROPARA. The experimental setup and a paraplegic subject of the experiment are presented in Fig.9 .
We have shown that in the cases where the acceleration and reference signal are similar, our algorithm is able to recognize sit-to-stand motion and to properly trigger leg stimulation at the desired instant. Also, we have showned that there is an influence of stimulation timing on applied hand forces during the motion. The best results were achieved for trials in which motion was similar to the one of the able bodied subjects in terms of trunk motion and the beginning of the leg motion with respect to the trunk acceleration signal.
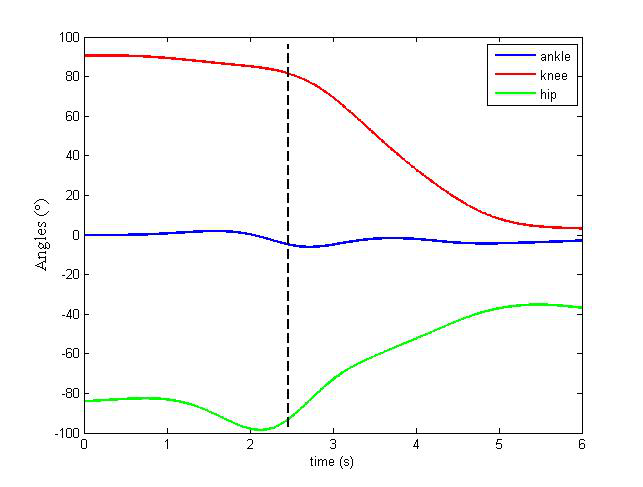
We also investigated dynamic optimization as a tool to improve FES assisted sit tostand transfers of paraplegic subjects. The objective would be to find optimal strategy for voluntary trunk movement, which would minimize hip, knee and ankle torques and demand minimal upper limb participation during the motion. Our results suggest paraplegic patients should bend their body forward in order to use linear momentum of the trunk in sit off phase. Figure 10 shows optimal coordination of ankle, knee, and hip angles during sit-to-stand motion [26] , [24] .
|
Signal-based segmentation of human locomotion using embedded sensor network
Participants : Maud Pasquier, Christine Azevedo Coste, Bernard Espiau, Christian Geny (CHU Montpellier), Fabien Jammes.
Last year, we introduced a simple approach to segment in homogeneous phases a long-duration record of locomotion data consisting of body segment acceleration and foot pressure information. We used a system based on a network of wireless nodes embedding various types of sensors [3] . Two cases were considered: walk and run around an indoor running track [35] and outdoor marathon [34] .
We now use this system as part of a study of mobility impairment caused by Parkinson's disease (fig.11 ). Freezing of gait (FOG) has been identified as one of the main contributors to gait disturbances in this disease. We introduce an ambulatory gait analysis method using body attached gyroscopes and accelerometers to detect the freezing of gait. One hand, we aim at proposing a FOG detection algorithm more robust because the existing algorithms were not able to detect the FOG without tremor. On the other hand, we would like to anticipate the freezing before ir is installed in order to reduce the risk of falling.
Before and during a FOG, a patient tends to walk slowly with short strides and fast rhythm. The detection of an increase of frequency is not enough, because there exists similar variations during the initiation of gait or a voluntary acceleration. The association of an increase of the gait rhythm together with a decrease of stride length allows us to detect a FOG. The computation of correlation coefficient in a moving window allows us to estimate the rhythm of strides. We are also working on different methods to estimate the stride length using one or two IMU (3-axis gyroscope and 3-axis accelerometer).
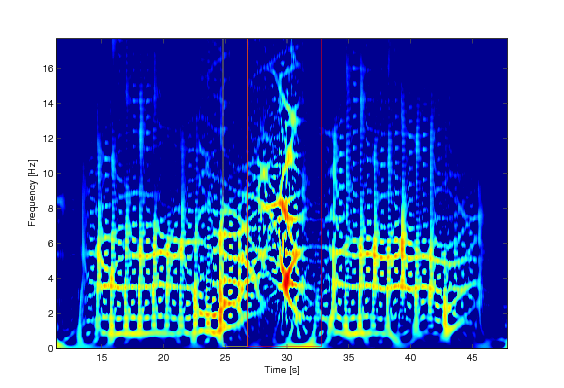
A time-frequency representation permits to show an increase of fundamental frequency and a duplication before a FOG, Fig.12 . The variations of the fundamental frequency are already detected with the correlation. In the future works, we aim at characterizing these duplications and to propose an algorithm of automatic detection.
Awake surgery: How to optimize functional brain mapping by improving per-operatory testing?
Participants : Cheikh Niang, Pom Charras, Stephane Argon, Christine Azevedo, Hugues Duffau, David Guiraud, François Bonnetblanc.
It is now possible to perform resections of slowgrowing tumors in awake patients. Using direct electrical stimulation (DES), real-time functional mapping of the brain can be used to prevent the resection of essential areas near the tumor. For now, simple clinical tests are performed on conscious patients and combined with DES in order to discriminate functional and non-functional areas invaded by the tumors. In this work we try to develop a simple device based on a simple technology to better quantify the performances of the patients during the surgery itself and give a real-time feedback to the neurosurgeon that will help to further guide the surgery by improving the sensibility of the functional mapping. This procedure should also allow building a strong database that should serve retrospectively to improve the surgical procedure and reinforce the neurosurgeons' experience as well as to monitor the patients' performances all along their life.
Closed-loop CoM based posture control in FES
Participants : Alejandro González, Mitsuhiro Hayashibe, Philippe Fraisse.
Center of Mass control has been used in humanoid robotics to create stable standing postures and movements. By controlling the CoM position and acceleration, joint trajectories which respect to the ZMP stability criterion can be generated. FES may be used to drive joint torques in order to maintain a standing posture within a closed loop controller. Current work is focused on locating a human's CoM by creating a statically equivalent serial chain (SESC) model using widely accessible equipment, such as the Kinect camera and the Wii balance board.